
It is a long walk from the entrance of the Korle Bu Teaching Hospital to the Public Health Nursing School, where the small office of the Non-Communicable Diseases Control Programme is based. The first time I visited, I had done enough reading on the imbalanced nature of funding of disease control in Ghana to not be surprised by the modest appearance. But others could be forgiven for expecting more from the hub of Ghana’s efforts to ensure that the burden of Non-Communicable Diseases (NCDs) or lifestyle diseases are “reduced to the barest minimum.”
To call the toll of lifestyle diseases on Ghanaians just burden, like a nuisance neck strain, is a bit of an understatement. It is more festering wound not too far from demanding an amputation. We have already crossed the threshold of alarming as far as lifestyle diseases are concerned.
Hypertension, stroke, diabetes and cancers are among the top 10 causes of death in Ghana and on the bigger canvas, NCDs are projected to become the commonest cause of death in sub-Saharan Africa by the year 2030.
The World Health Organisation (WHO) tells us lifestyle diseases were responsible for about 101,000 deaths in 2017, constituting 44 percent of deaths in Ghana.
This is up from five years prior, where WHO estimated that NCDs accounted for an estimated 34 percent of deaths and 31 percent of the disease burden in Ghana.
As part of the 2030 Agenda for Sustainable Development, WHO member States set the target of reducing early deaths from NCDs by a third.
The NCD Control Programme views data, which is collected by the Centre for Health Information Management (CHIM), as integral to any bid to reach this mark.
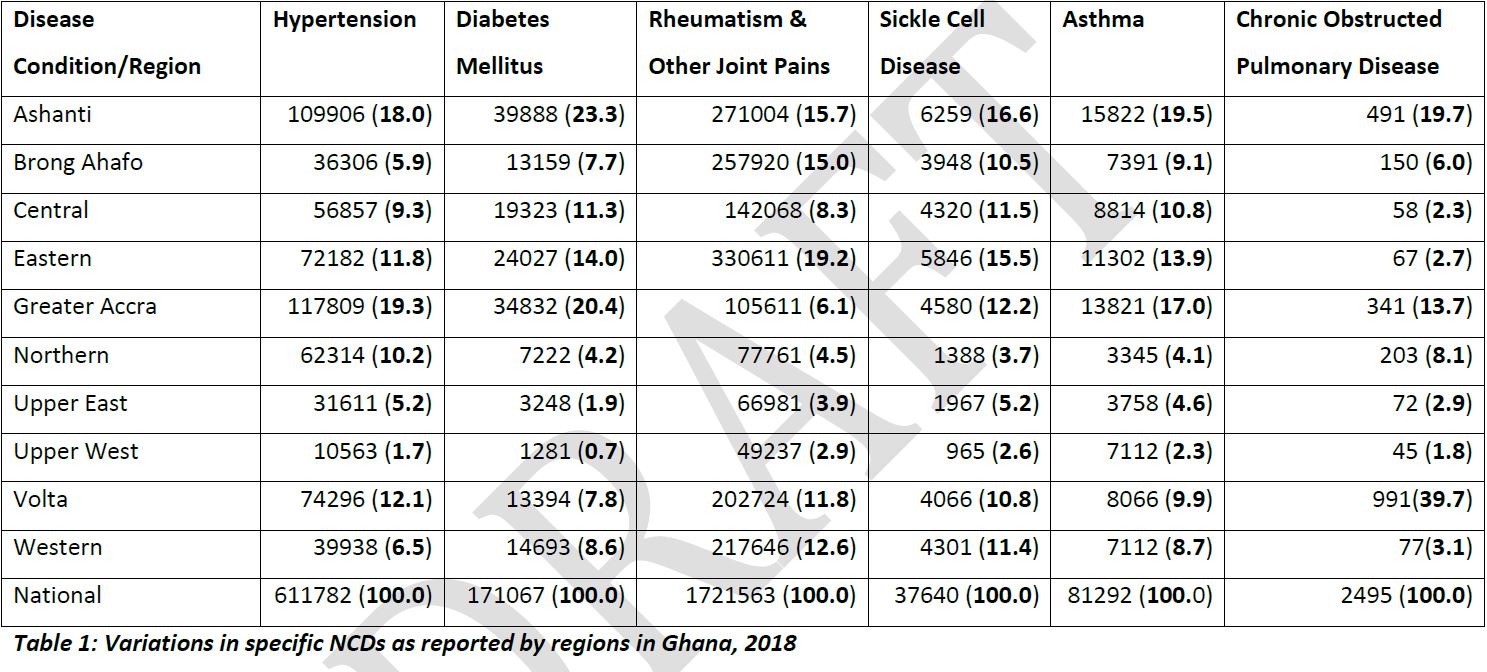
“The bulk” of the country’s health institutions are covered under the Ghana Health Service’s District Health Information System (DHIMSs) though “it’s not for the whole country,” the centre’s Programme Manager, Dr. Dennis Laryea said to me as we discussed the centre’s preliminary data on NCDs from 2018.
The system receives data from all public hospitals and some private health facilities.
Shying away from a definite percentage of health facilities covered, Dr. Laryea admitted he couldn’t “tell you what proportion of patients go to all the hospitals.”
But he finds some security in the fact “that a majority of the health facilities in Ghana are Ghana Health Service facilities.”
There are no real ideas when it comes to the coverage of the data being analysed. The lack of clarity continued as Dr. Laryea said the representation of data collected was “good enough” given the nuances of actual visits to health facilities.
“We would wish that every facility reports into this [District Health Information System] and there are efforts underway to make sure the private and teach hospitals also gather data.”
The challenges notwithstanding, the NCD Control Programme values the idea of making data one of its building blocks on the road to making Ghana a healthier nation.
Dr. Laryea’s outfit is currently reviewing data from 2013 to 2017 to ascertain hotspots for various lifestyle diseases and hoping for results by the end of 2019.
“What we’ve actually done now is to put all the five years together. Now we want to look at the individual areas and then map that with the facilities available.”
The thing with lifestyle diseases, though, is that they have actually worked hard to earn their moniker: the silent killers.
When it comes to killer diseases in Africa many people think of infectious diseases like tuberculosis, malaria, or even Ebola. But the reality is that diseases like cancer, diabetes and heart disease should be keeping more people up at night.
“Part of the problems with NCDs is that by the time you start seeing signs or going to the hospital for the diagnosis, a lot has happened in between,” reminded Dr. Laryea.
Thus, the long-term emphasis of the NCD Control Programme and its moves to harness data should ultimately be prevention.
“Our education, for example, doesn’t matter whether the person has a disease or not. It is targeted at the whole population,” Dr. Laryea said. In his view, given the rate of air pollution, the average diet and lack of exercise in Ghana, everybody is at risk.
Because of this, the NCD Control Programme is revising the NCD policy to include new guidelines for screening. The Programme hopes to have an army of wellness clinics to get ahead of the lifestyle diseases growing shadow.
“What we don’t have is a national guideline for screening,” remarked Dr. Laryea. “Part of it will also be looking at people who are at risk and screening them to determine if they are at the early stages of the disease and that will be better.”
As an additional step, the programme hopes it can “get the National Health Insurance Scheme to pay for those [screening] services so that people can go for them.”
But if my previous interactions with the programme are anything to go by, it will only get as far as its budget dictates.
In 2018, Dr. Laryea’s deputy, Dr. Efua Commey highlighted the funding concerns.
“…when it comes along funding lines, there is more funding allocated to the infectious diseases because they are more dramatic. It takes a really short time for people to come out with the diseases and the outcomes are really poor. But for chronic diseases, sometimes it takes decades.”
The NCD Programme’s preliminary data for 2018 fall in line with the gloomy estimates observers have made. It is estimated that there will be about 3.9 million deaths from these diseases in Africa by 2020.
In the most ideal situations, data, when harnessed effectively extends beyond the bare figures of cases recorded. The metadata of cases recorded could also give insight into why a particular clinic may be underserving its community and what diseases need to be prioritised.
For instance, a diabetes check-up should take into account records of a persons blood sugar over a period of time or a hypertensive patient would have the dietary regiment in a system along with the information that has to do with the patient’s blood pressure trends and medication doses.
One could be forgiven for having limited faith in data collection. Health system information in Ghana is lacking just like in many developing countries, including many in sub-Saharan Africa.
The Lancet Diabetes & Endocrinology in a 2016 publication highlighted some struggles that spread beyond countries like Ghana when it comes to collecting data on NCDs.
“…NCD data is either not collected at all or, if collected, is not released because of various systemic dysfunctions.”
At the very least, Ghana can release such data as evidenced by the NCD Programme’s annual report. Indications are that it intends to “track and interact with all citizens by sharing and linking routine information about population demographics and health services,” as Lancet suggests.
But Lancet also described as a problem the navigation of patients “between the public and private health-care sector” although, to Ghana’s credit, there is some semblance of a reporting framework in the form of the District Health Information System, which covers some private health facilities.
The shortage of databases in Africa has been described as acute. There are only 25 cancer registries that track cancer cases, according to a 2014 survey by the International Journal of Cancer. These only cover 18 out of 52 countries. Ghana thankfully has one
This is one of the reasons why WHO estimates that only one in five low and middle-income countries has the necessary data to guide cancer policy and planning. This most likely translates to other NCDs given the rising numbers.
Ghana’s healthcare system is still grappling with the basics. The long list of abandoned hospitals and the no bed syndrome are reminders of this. There’s the temptation to regard an investment in data as tertiary to Ghana’s health needs. But measuring the performance of health systems should become a priority for Ghana given how it could guide policy, improve accountability and take us closer to our healthcare goals.










{kind=link}